The Pediatric Symptom Checklist (PSC) is a brief screening questionnaire used by pediatricians and other health professionals to recognize psychosocial problems and improve treatment in children.
FREE

The Pediatric Symptom Checklist (PSC) is a brief screening questionnaire used by pediatricians and other health professionals to recognize psychosocial problems and improve treatment in children. It can be filled out in the office, at check-in, or before the visit.
There are checklist surveys available for parents/children and adolescent ages and in a variety of languages.
From Massachusetts General Hospital website:
“The Pediatric Symptom Checklist (PSC) is a brief questionnaire that helps identify and assess changes in emotional and behavioral problems in children. The PSC covers a broad range of emotional and behavioral problems and is meant to provide an assessment of psychosocial functioning…
Psychosocial problems are relatively common, affecting about 12% of children. Such problems often go unnoticed by pediatricians, teachers and even parents and can lead to more serious problems in later life. Research shows that earlier detection and treatment can lead to better outcomes. As such, professional organizations like the American Academy of Pediatrics recommend psychosocial screening as a part of the annual physical for all children and adolescents, and the country’s largest health insurer of children requires it.
The PSC is one of the most widely used screening tools for this purpose. It is an easy-to-use tool that is broadly valid and reliable. The PSC helps meet a growing array of therapeutic, research and administrative assessment needs in a wide range of clinical, educational and public health settings.”
Languages Available:
* Translations were created for the California Department of Health Services.
Online Versions of the PSC
There are also online versions that require a login.
Mental Health America provides the PSC with online score reports for free:
Information for Pediatric Clinicians
The Pediatric Symptom Checklist (PSC) helps pediatricians and pediatric nurse practitioners improve the recognition of psychosocial problems in their patients. The PSC is designed to fit into the workflow of a primary care practice and can be used to alert families of psychosocial and emotional issues.
When a large number of problems are detected, the clinician should assess further and decide whether watchful waiting or additional evaluation, referral and treatment is most appropriate.
When to Complete the PSC
The PSC can be administered at any point in pediatric care, but most practices opt to screen yearly during well-child visits.
The PSC can be administered in a number of ways:
Interpreting PSC Scores
Each item on the PSC receives zero, one or two points, with the scores on all 35 items summed for the total score. The recommended cutoff to indicate a possible problem is based on a large national sample in the U.S., where a score of 28+ identifies about 12% of children as being at risk (Jellinek et al., 1999; Murphy et al., 2016). Other studies support different cut-off points for other patient populations (eg.,Ishizaki, et al., 2000).
In practices that administer the PSC through an EMR or platform like CHADIS (Comprehensive Health and Decision Information System), the PSC total and subscale scores are calculated automatically. In practices using paper forms, clinicians may score the PSC themselves during review, while in others the medical assistant does the scoring. Scoring procedures can be found below.
Five to 20% of scores are above the cutoff point in most populations. This range reflects the fact that economic and cultural factors impact psychosocial functioning and reporting. For example, poverty is a major stressor that increases the percentage of children with positive scores (Jellinek et al., 1999). This reflects the reality that the burden of psychosocial dysfunction is higher for families living in poverty and experiencing greater social stress. In some cultures, parents may not feel comfortable acknowledging or emphasizing psychosocial issues and, as such, the entire bell-shaped distribution of scores and rate of positives may be shifted toward lower scores.
Steps After Screening
It is important to emphasize that the PSC is not designed to produce a diagnosis or to serve as a direct conduit to a specific treatment or medication. Instead it is meant to provide clinicians with suggestions for which patients may be at higher than average risk and with scores to compare to normative data.
Normal Range Scores
If the child’s score is within the expected normal range, you may be more confident turning your attention to other important but non-acute issues like anticipatory guidance, safety or other parental concerns.
Positive Screening Scores
If the total score or one of the sub-scale scores is in the “at-risk” range, most practices ask clinicians to devote a few extra minutes to getting a sense of why the number of problems reported is so high. Some clinicians discuss the symptoms that were marked as “often” with the parent and/or child, while others ask about major areas of daily functioning such as family, school, friends, activities and mood.
Some practices suggest that all positively screened children be offered a visit for a follow-up evaluation by a mental health professional, especially if one is readily available, while others recommend scheduling a follow-up appointment for further evaluation with the pediatrician in a week to a few months. Whatever the approach, next steps should be determined together by the parents and the clinician.
Many children who score positive may already be in therapy or have parents who do not want therapy, so it is often wisest to let parents know that a positive score indicates a high level of risk and that further assessment is probably warranted, but not mandatory.
For many children, a watchful waiting approach is also an option. This provides time to see whether problems diminish and gives parents a chance to consider next steps. Most children who screen positive on the PSC are positive again six or 12 months later. Parents who are reluctant to seek help initially may be more willing if they see that problems persist.
See the After Screening section for more information on recording scores and talking with parents.
Caveats and Possible Issues
The goal of screening with the PSC is to provide earlier intervention for children and adolescents who would benefit and prevent evolving childhood conditions from becoming more severe.
Understanding the PSC Report
The PSC is used primarily to screen children for overall emotional and behavioral problems using a scoring system. The cut-off scores used in the screening were established using large samples of children and adolescents.
Scores that indicate risk differ depending on your child’s age:
Children ages 6-17
Children ages 3-5
Scores on elementary school-related items 5, 6, 17 and 18 are ignored. Total score is based on the 31 remaining items.
https://www.massgeneral.org/psychiatry/treatments-and-services/pediatric-symptom-checklist
Physicians and other professionals should seek training from a licensed mental health professional to establish confidence in administering this tool. Ensure your office has procedures and ongoing training regarding what to do if a parent or child needs additional mental health support.
Tool can be downloaded and printed freely but may require permission to use commercially.
No Wrong Door Marketplace materials or resources are reviewed and curated by the Ohio School-Based Center of Excellence for Prevention & Early Intervention. To discuss resources, add, or suggest updates to No Wrong Door Marketplace, please call 513-529-2450. www.OhioSBCOE.org
The Pediatric Symptom Checklist (PSC) is a brief screening questionnaire used by pediatricians and other health professionals to recognize psychosocial problems and improve treatment in children. It can be filled out in the office, at check-in, or before the visit.
There are checklist surveys available for parents/children and adolescent ages and in a variety of languages.
From Massachusetts General Hospital website:
“The Pediatric Symptom Checklist (PSC) is a brief questionnaire that helps identify and assess changes in emotional and behavioral problems in children. The PSC covers a broad range of emotional and behavioral problems and is meant to provide an assessment of psychosocial functioning…
Psychosocial problems are relatively common, affecting about 12% of children. Such problems often go unnoticed by pediatricians, teachers and even parents and can lead to more serious problems in later life. Research shows that earlier detection and treatment can lead to better outcomes. As such, professional organizations like the American Academy of Pediatrics recommend psychosocial screening as a part of the annual physical for all children and adolescents, and the country’s largest health insurer of children requires it.
The PSC is one of the most widely used screening tools for this purpose. It is an easy-to-use tool that is broadly valid and reliable. The PSC helps meet a growing array of therapeutic, research and administrative assessment needs in a wide range of clinical, educational and public health settings.”
Languages Available:
* Translations were created for the California Department of Health Services.
Online Versions of the PSC
There are also online versions that require a login.
Mental Health America provides the PSC with online score reports for free:
Information for Pediatric Clinicians
The Pediatric Symptom Checklist (PSC) helps pediatricians and pediatric nurse practitioners improve the recognition of psychosocial problems in their patients. The PSC is designed to fit into the workflow of a primary care practice and can be used to alert families of psychosocial and emotional issues.
When a large number of problems are detected, the clinician should assess further and decide whether watchful waiting or additional evaluation, referral and treatment is most appropriate.
When to Complete the PSC
The PSC can be administered at any point in pediatric care, but most practices opt to screen yearly during well-child visits.
The PSC can be administered in a number of ways:
Interpreting PSC Scores
Each item on the PSC receives zero, one or two points, with the scores on all 35 items summed for the total score. The recommended cutoff to indicate a possible problem is based on a large national sample in the U.S., where a score of 28+ identifies about 12% of children as being at risk (Jellinek et al., 1999; Murphy et al., 2016). Other studies support different cut-off points for other patient populations (eg.,Ishizaki, et al., 2000).
In practices that administer the PSC through an EMR or platform like CHADIS (Comprehensive Health and Decision Information System), the PSC total and subscale scores are calculated automatically. In practices using paper forms, clinicians may score the PSC themselves during review, while in others the medical assistant does the scoring. Scoring procedures can be found below.
Five to 20% of scores are above the cutoff point in most populations. This range reflects the fact that economic and cultural factors impact psychosocial functioning and reporting. For example, poverty is a major stressor that increases the percentage of children with positive scores (Jellinek et al., 1999). This reflects the reality that the burden of psychosocial dysfunction is higher for families living in poverty and experiencing greater social stress. In some cultures, parents may not feel comfortable acknowledging or emphasizing psychosocial issues and, as such, the entire bell-shaped distribution of scores and rate of positives may be shifted toward lower scores.
Steps After Screening
It is important to emphasize that the PSC is not designed to produce a diagnosis or to serve as a direct conduit to a specific treatment or medication. Instead it is meant to provide clinicians with suggestions for which patients may be at higher than average risk and with scores to compare to normative data.
Normal Range Scores
If the child’s score is within the expected normal range, you may be more confident turning your attention to other important but non-acute issues like anticipatory guidance, safety or other parental concerns.
Positive Screening Scores
If the total score or one of the sub-scale scores is in the “at-risk” range, most practices ask clinicians to devote a few extra minutes to getting a sense of why the number of problems reported is so high. Some clinicians discuss the symptoms that were marked as “often” with the parent and/or child, while others ask about major areas of daily functioning such as family, school, friends, activities and mood.
Some practices suggest that all positively screened children be offered a visit for a follow-up evaluation by a mental health professional, especially if one is readily available, while others recommend scheduling a follow-up appointment for further evaluation with the pediatrician in a week to a few months. Whatever the approach, next steps should be determined together by the parents and the clinician.
Many children who score positive may already be in therapy or have parents who do not want therapy, so it is often wisest to let parents know that a positive score indicates a high level of risk and that further assessment is probably warranted, but not mandatory.
For many children, a watchful waiting approach is also an option. This provides time to see whether problems diminish and gives parents a chance to consider next steps. Most children who screen positive on the PSC are positive again six or 12 months later. Parents who are reluctant to seek help initially may be more willing if they see that problems persist.
See the After Screening section for more information on recording scores and talking with parents.
Caveats and Possible Issues
The goal of screening with the PSC is to provide earlier intervention for children and adolescents who would benefit and prevent evolving childhood conditions from becoming more severe.
Understanding the PSC Report
The PSC is used primarily to screen children for overall emotional and behavioral problems using a scoring system. The cut-off scores used in the screening were established using large samples of children and adolescents.
Scores that indicate risk differ depending on your child’s age:
Children ages 6-17
Children ages 3-5
Scores on elementary school-related items 5, 6, 17 and 18 are ignored. Total score is based on the 31 remaining items.
https://www.massgeneral.org/psychiatry/treatments-and-services/pediatric-symptom-checklist
Physicians and other professionals should seek training from a licensed mental health professional to establish confidence in administering this tool. Ensure your office has procedures and ongoing training regarding what to do if a parent or child needs additional mental health support.
Tool can be downloaded and printed freely but may require permission to use commercially.
No Wrong Door Marketplace materials or resources are reviewed and curated by the Ohio School-Based Center of Excellence for Prevention & Early Intervention. To discuss resources, add, or suggest updates to No Wrong Door Marketplace, please call 513-529-2450. www.OhioSBCOE.org
Only logged in customers who have purchased this product may leave a review.

SAMHSA compiled this fact sheet about the importance of parents and caregivers having age-appropriate conversations about alcohol and other drugs with their kids.
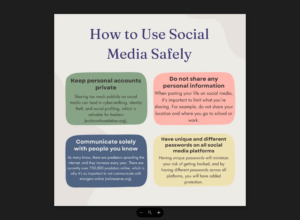
This Cyber Safety graphic was created by high school students as part of their youth-led prevention project.
Video with discussion guide for 5 research-backed strategies for schools to consider as they partner with families for student mental health and well-being.

Mental Health America created this downloadable form that adults can use to get ready for a conversation about mental health with your doctor.
Reviews
There are no reviews yet.